





Sharon has 21+ years of experience as a qualified Emergency Care Nurse registered with the Australian Health Practitioner Regulation Agency (APHRA) and 12+ years as a First Aid Trainer.
She takes pride in FirstAidPro making first aid training available, comprehensive and affordable to everybody.
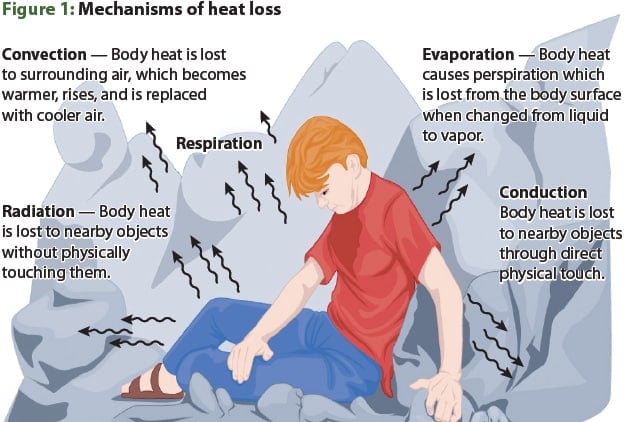
Hypothermia is a medical emergency that occurs when the body’s core temperature drops below 35°C, impairing normal function and, if untreated, causing cardiac arrest and death. Whether triggered by prolonged exposure to cold air, cold-water immersion, or as a complication of serious illness or injury, accidental hypothermia can affect anyone — from bushwalkers caught in an unexpected alpine storm to elderly Australians sitting in an unheated home through winter. Understanding the causes, recognising the signs and symptoms of hypothermia, and knowing how to deliver correct prehospital first aid can mean the difference between a full recovery and a tragedy.
This article explains what hypothermia is, how it progresses through three clinically distinct stages, what the recommended emergency treatment looks like, and what bystanders and first responders can do before paramedics arrive.
Ready to respond with confidence? First Aid Pro’s nationally recognised first aid courses teach you to manage medical emergencies like hypothermia, cardiac arrest and other common injuries using the latest Australian Resuscitation Council guidelines.

Key Takeaways
- Hypothermia is defined as a core body temperature below 35°C.
- It can develop even in mild Australian weather — particularly during cold-water immersion.
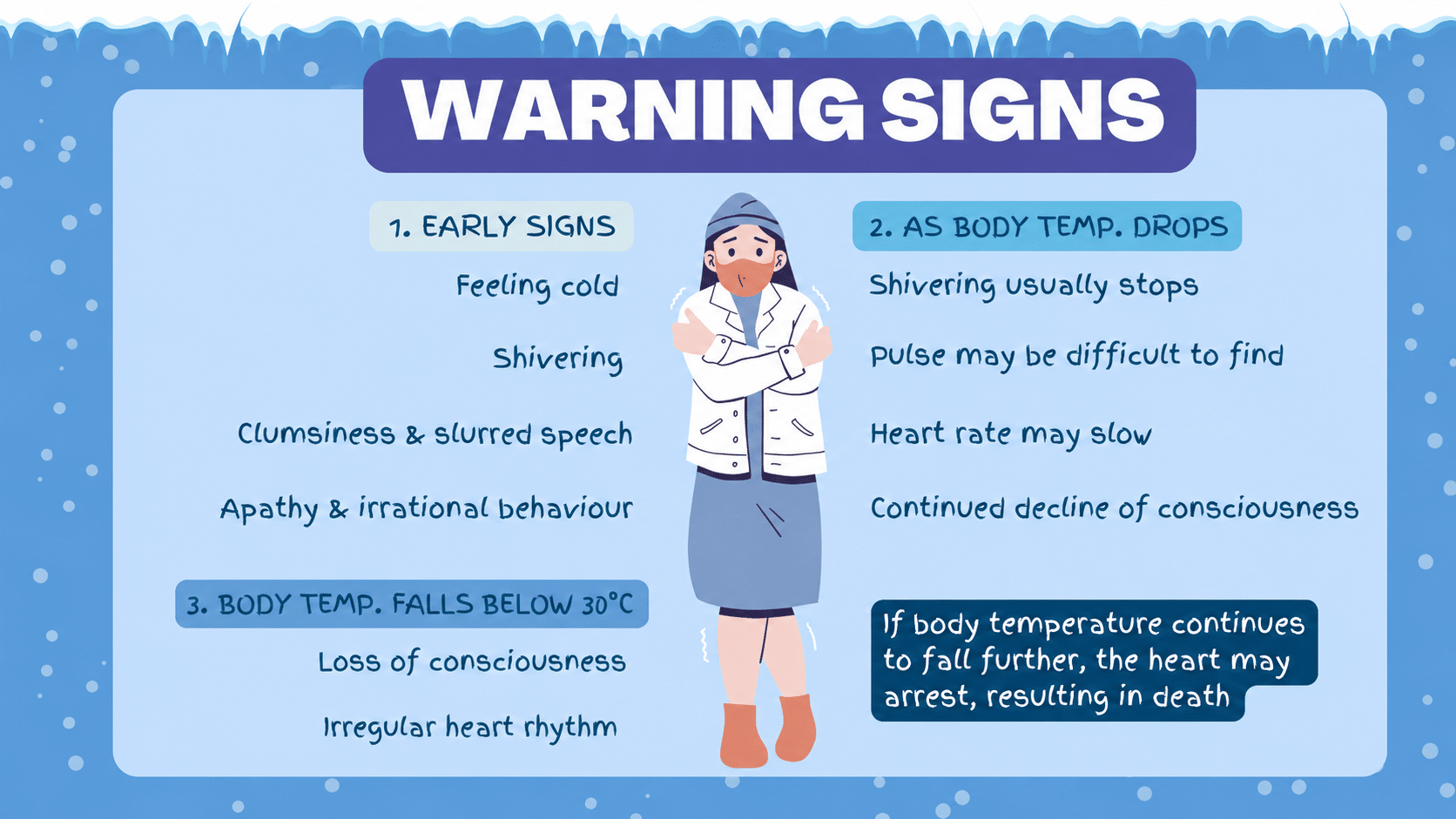
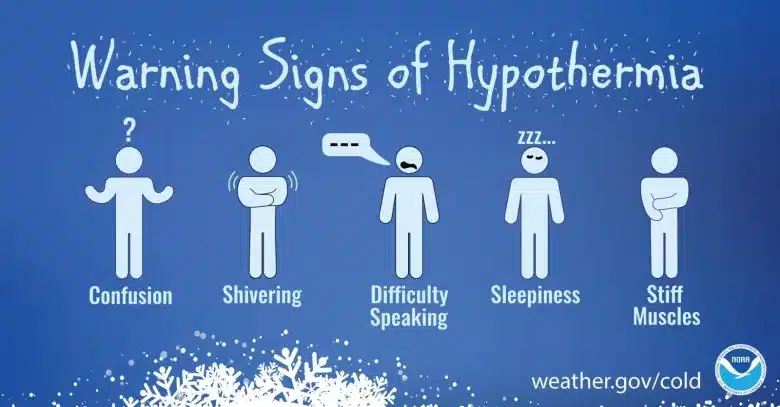
- The earliest signs include uncontrolled shivering, pale skin, slurred speech and confusion.
- Shivering that suddenly stops in a cold environment is a warning sign of deterioration.
- The correct first aid response prioritises preventing further heat loss and gentle rewarming — never vigorous rubbing or direct heat.
- Call Triple Zero (000) for any suspected moderate or severe hypothermia.
- Hypothermic cardiac arrest is potentially reversible — do not stop CPR until told to do so by paramedics or a medical officer.
What Is Hypothermia? Definition and Overview
The human body functions optimally within a narrow temperature range of approximately 36.1°C to 37.2°C. When the core body temperature — measured at the oesophagus, rectum, or bladder rather than the skin surface — falls below 35°C, the body’s physiological balance begins to break down. This condition is what clinicians define as hypothermia.
It is important to distinguish between feeling cold (a normal, temporary sensation the body manages effectively) and being hypothermic (a pathological state in which heat loss outpaces the body’s capacity for heat production). The latter is a genuine medical emergency requiring prompt action.
Primary hypothermia arises directly from exposure to cold environments — cold air, wind, rain, or water — in an otherwise healthy individual. Secondary hypothermia occurs as a consequence of another medical condition, such as sepsis, hypothyroidism, severe hypoglycaemia, major trauma, or significant burns, which impair the body’s normal thermoregulatory reflexes.
How Common Is Hypothermia in Australia?
Australia is not immune to hypothermia. While its tropical north is rarely at risk, the alpine regions of New South Wales, Victoria, and the Australian Capital Territory see genuine cold-weather emergencies every year. Cold-water immersion in coastal and inland waterways — which can cause hypothermia even when air temperatures are mild — is a significant risk factor year-round. High-risk groups in the Australian context include:
- Elderly people (declining thermoregulation and reduced vasoconstriction reflex)
- Infants and young children
- People experiencing homelessness
- Outdoor workers and recreational users in alpine, rural or marine environments
- People affected by alcohol or drug use (alcohol causes vasodilation, accelerating heat loss)
- Patients with trauma, sepsis or other acute illness in the prehospital phase
Accidental Hypothermia: Causes and Risk Factors
Accidental hypothermia is the unintentional drop of core temperature below 35°C. It arises when the rate of heat loss exceeds the rate of heat production, and the body’s compensatory mechanisms — primarily shivering and vasoconstriction — can no longer keep pace.
Environmental Causes
The most direct cause is prolonged exposure to cold. Water conducts heat away from the body approximately 25 times faster than air at the same temperature, which is why cold-water immersion represents one of the fastest routes to severe hypothermia. Wind dramatically accelerates heat loss through convection, even at temperatures well above freezing. Rain-soaked clothing provides almost no insulation, magnifying the risk.
Medical and Physiological Risk Factors
Several conditions impair the body’s ability to generate or retain heat:
Risk Factor | Mechanism |
Advanced age | Decreased heat production; impaired vasoconstriction and shivering reflex |
Alcohol and drug intoxication | Vasodilation increases heat loss; impairs judgement about the environment |
Malnutrition and low body fat | Reduced metabolic heat production and insulation |
Hypothyroidism | Decreased metabolic rate and heat production |
Sepsis | Impairs thermoregulation; causes abnormal vasodilation |
Trauma (especially with haemorrhage) | Blood loss reduces perfusion; immobility prevents heat production |
Certain medications | Sedatives, antidepressants, antihypertensives and antipsychotics can impair thermal regulation |
Hypoglycaemia | Reduced energy substrate for heat production |
Situational and Occupational Causes
Outdoor recreation — hiking, skiing, kayaking, open-water swimming — carries real risk, particularly when plans change, equipment fails, or weather closes in unexpectedly. In the prehospital context, trauma management must always account for hypothermia, as injured patients cool rapidly even in subtropical environments. Prolonged surgical procedures and time spent on a cold ground surface also contribute to secondary hypothermia in clinical settings.
Hypothermia Clinical Manifestations: The Three Stages
Clinicians and emergency medicine practitioners classify hypothermia into three stages based on core temperature, each with distinct clinical manifestations. In the field, where precise temperature measurement is rarely possible, the Swiss Staging System (HT I–IV) — endorsed by the International Commission for Mountain Emergency Medicine (ICAR MedCom) — guides prehospital assessment based on observable signs and symptoms rather than thermometer readings alone.
📊 The Three Stages of Hypothermia at a Glance
Stage | Core Temperature | Key Signs |
Mild (HT I) | 32°C – 35°C | Shivering, cold pale skin, confusion, clumsiness |
Moderate (HT II) | 28°C – 32°C | Shivering stops, drowsiness, slow pulse, loss of coordination |
Severe (HT III–IV) | Below 28°C | Unconsciousness, absent or faint pulse, cardiac arrest risk |
Stage 1 – Mild Hypothermia (32°C to 35°C)
In the mild stage, the body is still actively fighting to maintain its core temperature. Shivering is the hallmark sign — it is the body’s primary mechanism for generating heat through involuntary muscle contraction. Other signs and symptoms of mild hypothermia include:
- Rapid heart rate and breathing rate
- Pale, cool skin; goosebumps
- Poor coordination and clumsiness
- Slurred speech
- Mild confusion or forgetfulness
- Irritability or unusual behaviour
A useful clinical memory tool for the early stage is the “umbles”: the person stumbles, mumbles, fumbles and grumbles. A person in mild hypothermia is usually still conscious and responsive, which creates a window for effective first aid.

Stage 2 – Moderate Hypothermia (28°C to 32°C)
As core body temperature continues to fall into the moderate range, the body begins to lose the battle. One of the most dangerous and deceptive signs is that shivering stops — not because the person is warming up, but because the muscles are no longer capable of generating heat. Other clinical manifestations include:
- Progressively worsening confusion and disorientation
- Extreme fatigue and drowsiness
- Significantly slowed heart rate (bradycardia)
- Slow, shallow breathing
- Muscle stiffness and rigidity
- Bluish discolouration of the skin (cyanosis)
- Possible loss of consciousness
Cardiac arrhythmias, including atrial fibrillation, become increasingly likely as the heart muscle cools. The QRS complex widens on an ECG, and J-waves (Osborn waves) may appear — a characteristic ECG abnormality of hypothermia.
Stage 3 – Severe Hypothermia (Below 28°C)
Severe accidental hypothermia carries a high risk of hypothermic cardiac arrest. Ventricular fibrillation — a chaotic, disorganised cardiac rhythm incompatible with effective circulation — becomes the predominant arrhythmia risk below approximately 28°C. Signs include:
- Unconsciousness or unresponsiveness
- Fixed and dilated pupils (which alone should NOT be interpreted as a sign of death in a hypothermic patient)
- Very faint or absent pulse
- Absent or barely perceptible breathing
- Extreme muscle rigidity
- Skin that may appear mottled or deeply cyanosed
The critical clinical principle in severe hypothermia is: “No one is dead until they are warm and dead.” Successful resuscitation of patients with core temperatures below 20°C has been documented in the medical literature. Defibrillation is generally withheld until the core temperature rises above 30°C, as the hypothermic heart tends to be resistant to defibrillation until rewarmed.
Signs and Symptoms of Hypothermia: Quick-Reference Summary
🔴 Physical Signs
- Shivering — present in mild hypothermia; absent in moderate-to-severe hypothermia, which is a danger sign
- Cold, pale, or blue-tinged skin
- Weak, slow or absent pulse
- Slow, shallow or absent breathing
- Muscle rigidity or stiffness
- Fixed and dilated pupils in severe cases
🔴 Behavioural and Cognitive Symptoms
- Confusion, disorientation, or memory lapses
- Slurred speech
- Poor coordination or stumbling
- Paradoxical undressing — a late sign in severe cases where the person removes clothing due to a distorted sensation of warmth
- Progressive drowsiness leading to unconsciousness
When to Suspect Hypothermia
If a person has been exposed to cold — whether cold air, cold water, wind and rain, or even a cold floor for a prolonged period — and they display any of the above signs and symptoms, treat the situation as hypothermia until proven otherwise. Do not wait for a thermometer reading. Call Triple Zero (000) if the person is confused, drowsy, has stopped shivering in a cold environment, or is unresponsive.
Management of Hypothermia: Prehospital First Aid
Effective prehospital management of hypothermia follows a clear sequence. The primary goals are to prevent further heat loss, support vital functions, and facilitate safe transfer to the emergency department. Rough handling must be avoided at all times, as it can precipitate ventricular fibrillation in an already irritable hypothermic heart.
Step-by-Step Prehospital First Aid for Hypothermia
Step 1 — Ensure scene safety and call for help Do not put yourself at risk. Call Triple Zero (000) immediately for moderate or severe hypothermia. Provide your location, the person’s condition, and estimated time of exposure.
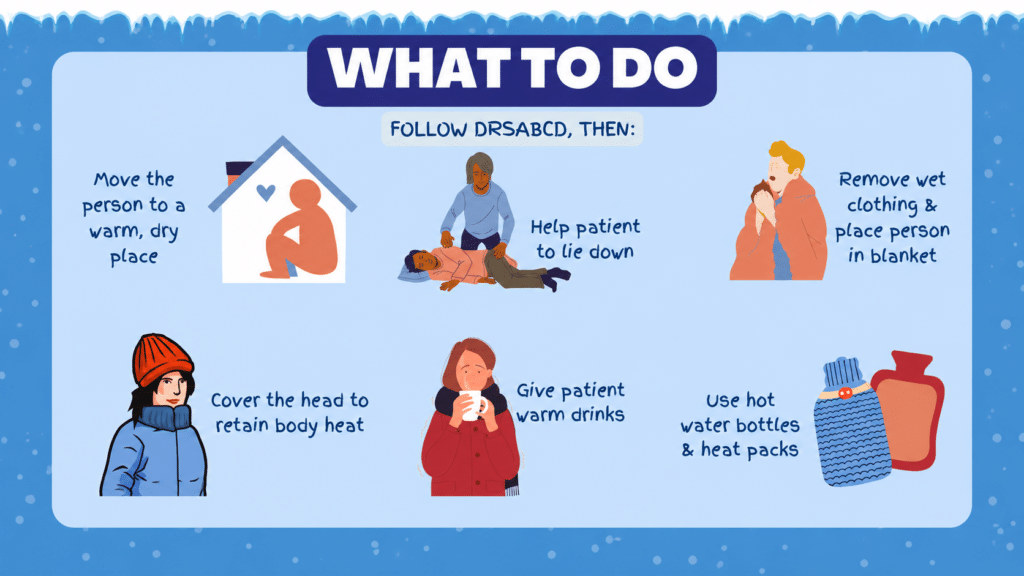
Step 2 — Move to shelter Remove the person from the cold environment. Protect them from wind, rain and ground cold. Place an insulating layer (sleeping mat, bag, clothing) beneath them to reduce conductive heat loss to the ground.
Step 3 — Remove wet clothing — gently Wet clothing accelerates heat loss. Remove it carefully and slowly, supporting all limbs. Never jostle or manoeuvre the person aggressively.
Step 4 — Prevent further heat loss Cover the person with dry blankets, sleeping bags, or a vapour barrier. Include the head — a significant portion of heat loss occurs from the scalp. In wilderness settings, an insulated “hypothermia wrap” using a sleeping bag and weatherproof outer layer is the recommended rewarming technique.
Step 5 — Apply gentle external rewarming Place warm packs or warm water bottles wrapped in cloth at the armpits, groin, and sides of the neck — areas where large blood vessels run close to the skin surface. Do not apply heat directly to the skin. Do not use electric blankets or radiant heat sources without medical supervision.
Step 6 — If conscious: warm fluids If the person is alert, able to sit up, and able to swallow safely, offer warm (not hot) non-alcoholic fluids. Warm sweet drinks provide both fluid and glucose to support heat production.
Step 7 — Monitor continuously Monitor their breathing, pulse, and level of consciousness until paramedics arrive. Keep them as still and as flat as possible.
⚠️ What NOT to Do
Incorrect Action | Why It Is Harmful |
Vigorously rub the limbs | Drives cold blood from the periphery to the heart, worsening arrhythmia risk |
Give alcohol | Accelerates vasodilation and heat loss; impairs judgement |
Apply direct heat (fire, hot water, uninsulated heat pack) | Causes burns and sudden peripheral vasodilation |
Allow the person to walk or exercise | Physical exertion in moderate-to-severe hypothermia can trigger cardiac arrest |
Assume fixed and dilated pupils mean death | Hypothermia causes pupils to appear fixed and dilated; this is not a reliable sign of death |
Train to respond — not just react. First Aid Pro delivers nationally recognised first aid training across Australia, covering CPR, and emergency medicine scenarios. Book your course with First Aid Pro today.
CPR in Hypothermic Cardiac Arrest
If a hypothermic patient is unresponsive and not breathing normally, commence CPR using DRSABCD immediately. In confirmed cardiac arrest due to hypothermia:
- Perform CPR continuously — do not stop until the patient reaches hospital or is declared dead by a medical officer after rewarming
- Defibrillation may be attempted up to three times if ventricular fibrillation is present, but if unsuccessful at low temperatures, defer further defibrillation until core temperature exceeds 30°C
- Epinephrine (adrenaline) and other cardiac arrest medications may be withheld or given at extended intervals, as drug metabolism is significantly slowed in hypothermic patients
- Intubation should be performed by trained personnel where airway management is required, but should not delay other resuscitation measures
The golden rule remains: continue resuscitation and life support until the patient is rewarmed.
Rewarming Techniques in the Field: A Practical Summary
🏔️ The Hypothermia Wrap Technique
What you need: Sleeping mat or tarp → dry clothing/blankets → sleeping bag → waterproof outer layer → hat
Sleeping mat, tarp, or folded clothing
Wrap around the body
Add a warm insulating layer
Block wind and moisture
Keep packs insulated — never apply direct heat to skin
Include a hat or wrap
Preventing Hypothermia: Practical Tips for Australian Conditions
Prevention is always preferable to treatment. Managing the risk of accidental hypothermia in Australian environments involves preparation, awareness, and the right gear.
- Dress in moisture-wicking layers — the inner layer moves sweat away from skin; the middle layer insulates; the outer layer blocks wind and water.
- Never rely on cotton in cold, wet conditions — cotton holds moisture against the skin and provides almost zero insulation when wet.
- Wear a hat and gloves — significant heat loss occurs from the head and extremities.
- Stay dry — change out of wet clothing as quickly as possible.
- Avoid alcohol before and during outdoor activities in the cold — it creates a false sense of warmth while accelerating heat loss.
- Plan and communicate — always advise someone of your route, destination and expected return time before heading into alpine or remote areas.
- Carry an emergency foil blanket in every first aid kit and backpack.
- Check on vulnerable people — elderly neighbours, homeless individuals, and young children are at elevated risk during cold spells.
- In the water: wear a wetsuit or drysuit for activities in water below 20°C, and a lifejacket on all watercraft.
Turn knowledge into life-saving skills. First Aid Pro offers nationally recognised first aid courses delivered by qualified trainers across Australia. Learn to perform CPR, and respond to medical emergencies with composure. Register with First Aid Pro and be ready when it counts.
Related Reading
- Paal P, Pasquier M, Darocha T, et al. Accidental Hypothermia: 2021 Update. International Journal of Environmental Research and Public Health. 2022;19(1):501. doi:10.3390/ijerph19010501
- Australian Resuscitation Council (ARC). Guideline 9.3.3 – Accidental hypothermia. ARC & New Zealand Resuscitation Council; 2021
- Emergency Care Institute – NSW Health. Hypothermia: Clinical Management Tool. NSW Agency for Clinical Innovation; Updated November 2024.
- Wilderness Medical Society. Practice guidelines for the out-of-hospital evaluation and treatment of accidental hypothermia. Wilderness & Environmental Medicine. 2019;30(4S):S47–S69.
- Better Health Channel: Hypothermia
Frequently Asked Questions
What is the difference between primary hypothermia and secondary hypothermia?
Primary hypothermia occurs when a previously healthy person is exposed to a cold environment and their body cannot maintain a normal core temperature. Secondary hypothermia develops as a complication of another underlying medical condition — such as sepsis, hypothyroidism, trauma, or hypoglycaemia — that disrupts normal thermoregulation. Both require urgent management, but secondary hypothermia also requires treatment of the underlying cause.
. Can you develop hypothermia in Australia during summer?
- Can you develop hypothermia in Australia during summer?
Yes. Cold-water immersion is the most common warm-weather cause. Ocean, river and lake temperatures in many parts of Australia remain well below 20°C year-round. Even in summer, a person who falls from a boat or is caught in a river current can become hypothermic within 30 to 60 minutes, depending on water temperature and physical condition. Wind and rain can also combine to cause hypothermia during mild-temperature conditions.
Is frostbite the same as hypothermia?
No. Hypothermia is a drop in core body temperature that affects the entire body. Frostbite is localised freezing of body tissue — most commonly affecting fingers, toes, ears and the nose — when skin and the layers below it freeze. The two conditions can occur simultaneously, and anyone with frostbitten extremities in a cold environment should also be assessed for hypothermia. Frostbitten tissue should never be rubbed, and rewarming should only occur once there is no risk of refreezing.
How long does recovery from hypothermia take?
Recovery time depends on severity. Mild hypothermia treated promptly with correct rewarming techniques typically resolves within a few hours with no lasting effects. Moderate hypothermia generally requires hospital admission and may take one to several days to fully resolve. Severe accidental hypothermia — particularly when it involves hypothermic cardiac arrest or ECLS — can require intensive care for days to weeks, and full neurological recovery can take considerably longer. The extent of any long-term effects depends on how long the brain and vital organs were deprived of adequate circulation.
When should I call Triple Zero (000) for hypothermia?
Call Triple Zero (000) immediately if the person: is confused, drowsy or losing consciousness; has stopped shivering in a cold environment; has a slow or absent pulse; is unresponsive or not breathing normally; or has been in cold water for any significant period. Do not delay calling for professional help while you provide first aid — both can happen at the same time.




